


ASV showed better control of respiratory events than CPAP in patients with CompSA
In an intention-to-treat analysis, success (apnea hypopnea index [AHI] < 10) at 90 days of therapy was achieved in 89.7% of patients treated with ASV versus 64.5% of participants treated with CPAP.1
[N = 66, prospective randomised trial]

ASV reduces residual sleepiness after APAP therapy in patients with mixed sleep apnea
After 30 days of APAP treatment, ASV provided a further reduction (compared to baseline) of 12.9% in AHI, 48.5% in central sleep apnea index (CSAI), 26.1% in micro-arousal index (MAI), and 37.9% in Epworth Sleepiness Scale (ESS) score at similar mean pressure.2
[N = 42, sequential study]

In a small retrospective analysis, ASV improved AHI and ESS in patients following acute ischaemic stroke
In opioid-induced CSA, ASV therapy reduced AHI by 84.7%, central apnea index (CAI) by 95.7%, apnea index (AI) by 96.4%, and respiratory arousal index (RAI) by 77.1% when compared to bi-level ST. Respiratory parameters were normalised in 83.3% of patients on ASV Auto, but only 33.3% of patients on bi-level ST.3
[N = 18, prospective, randomised crossover polysomnography study]

ASV improves AHI and ESS in post-acute ischemic stroke patients
ASV therapy improved outcomes for post-acute ischemic stroke patients with CSA, reducing AHI by 81.8% and ESS by 35.6%.4
[N = 15, single centre retrospective analysis]

A decade of evidence brings clarity to ASV
Since 2015 and the results of SERVE-HF,5 the indications for use of ASV therapy have been revised. According to ERS consensus statement from 2017,6 ASV should be prescribed in cases of persistent CSA with AHI ≥ 15 per hour despite CPAP treatment, except in patients with symptomatic heart failure (NYHA 2-4) with reduced left ventricular ejection fraction (LVEF ≤ 45%), and moderate to severe CSA.
The 2025 ERS/ESRS7 statement supports ASV is safe and effective for selected CSA patients with heart failure, except those with chronic, symptomatic heart failure (NYHA II–IV) and LVEF ≤ 45%, or moderate to severe central sleep apnea. ASV may be considered for other CSA types, including treatment-emergent, drug-induced, neurological, or idiopathic CSA. For symptomatic patients with LVEF 30–45% unresponsive to CPAP, ASV should only begin in expert centres with close specialist monitoring.
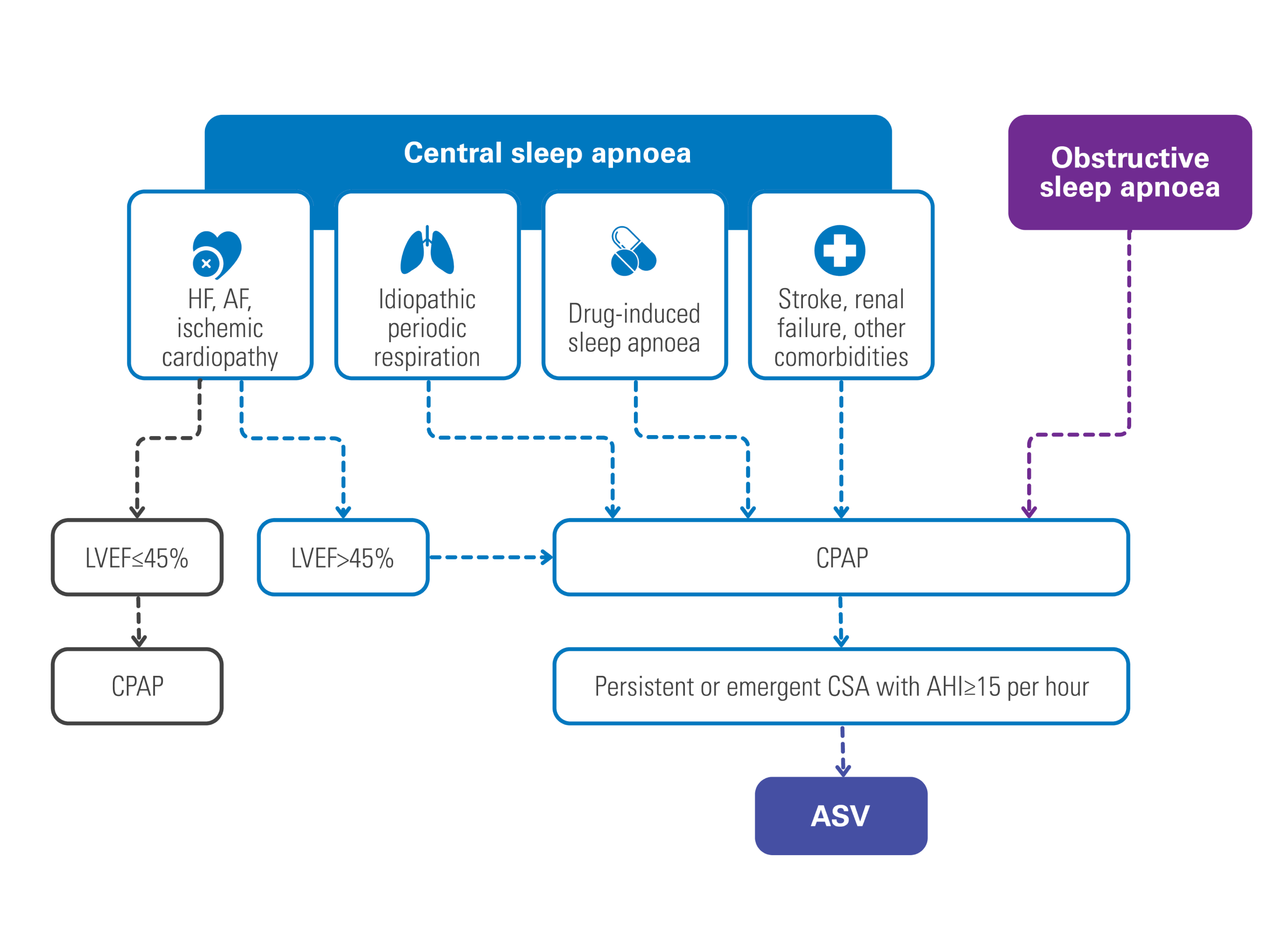
Adapted from the ERS and AASM statements about CSA.
READ-ASV registry: indications and benefits of ASV in real life
READ-ASV8, launched in 2017, looked at the clinical benefits of ASV therapy in 801 patients in real-life settings.
The findings from the READ-ASV study8 reveal that ASV therapy is primarily used in clinical practice for patients with treatment-emergent central sleep apnea (TE-CSA) and CSA with cardiovascular disease.
These patients experienced symptoms such as impaired quality of life, sleepiness, and low sleep quality, which were improved with ASV treatment, especially in individuals with pre-existing sleep disordered breathing (SDB).

CPAP, APAP and bilevel therapy
Positive airway pressure therapy can be delivered in a number of modes:
- Continuous positive airway pressure (CPAP), which delivers air at a fixed pressure.
- Automatic positive airway pressure (APAP), which automatically adjusts pressure levels based on a patient's breathing. APAP may be suitable for patients with REM-related sleep apnea, positional apnea or who experience non-compliance with standard CPAP therapy.
- Bilevel therapy, which provides higher inspiratory pressure (IPAP) and lower expiratory pressure (EPAP) - can also be effective for certain OSA patients who are non-compliant, and used to treat a wide-range of sleep and respiratory disordered breathing other than OSA such as include CSA, overlap syndrome, COPD, and more.

Patient outcomes and comorbidities
Helping your patients start and continue with the most effective sleep apnea treatment can help them regain control of their lives. Effective treatment has been shown to reverse the effects of daytime sleepiness, fatigue, moodiness and depression. And studies have shown that when patients are successful with their therapy, their long-term health care costs are at least 50% lower overall.1
There are also a variety of serious comorbidities such as cardiovascular disease, diabetes and stroke that have a strong connection to sleep apnea.
FACE registry: adopting a phenotyping approach with ASV
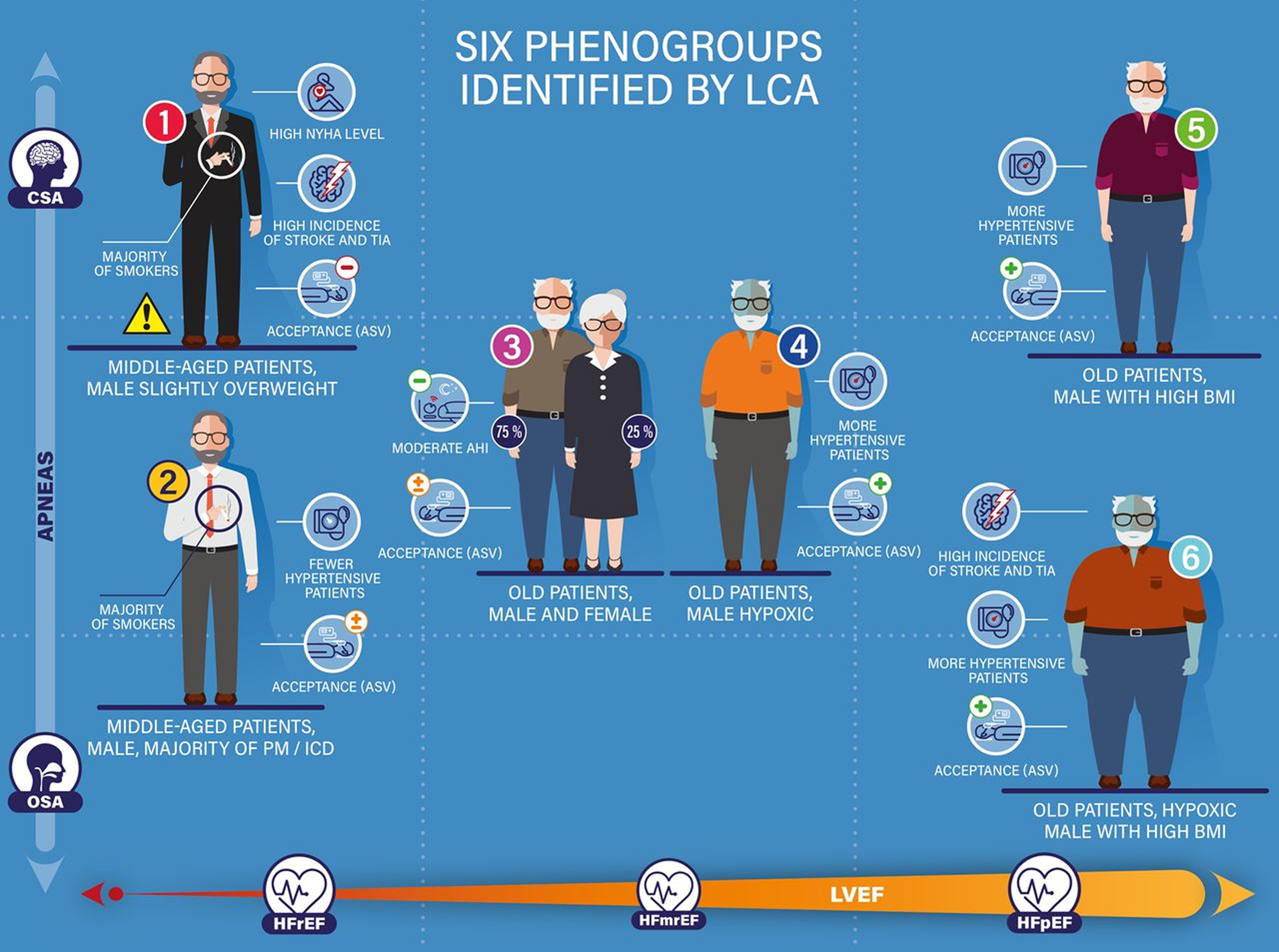
The FACE registry9,10 enrolled 503 heart failure patients from 2009 to 2018, with reduced ejection fraction before 2015, and then with preserved ejection fraction only after 2015. Among the 324 patients who underwent the two years follow-up, the analysis distinguished six phenogroups of patients and highlighted the existence of various phenotypes in chronic heart failure patients eligible for ASV therapy.
Results have shown that, compared to ASV non-users, three phenotypes had a better prognosis on morbi-mortality with ASV treatment: namely patients with HFmrEF/HFpEF (heart failure with mid-range ejection fraction/heart failure with preserved ejection fraction); patients with obstructive sleep apnea (OSA) or CSA-OSA; and patients who are older, male and obese. The phenotype that benefited the most included older, obese, hypoxic and hypertensive patients.
ASV videos: watch experts talking about ASV therapy

Professor Michael Arzt, Professor of Internal Medicine, Regensburg, Germany speaks on what evidence-based medicine says about ASV therapy.

How to treat your patients with central sleep apnea
Discover how Resmed adaptive servo-ventilation (ASV)* solution promotes harmony, safety and comfort.

More about treatment options

Treatment options for CSA
