


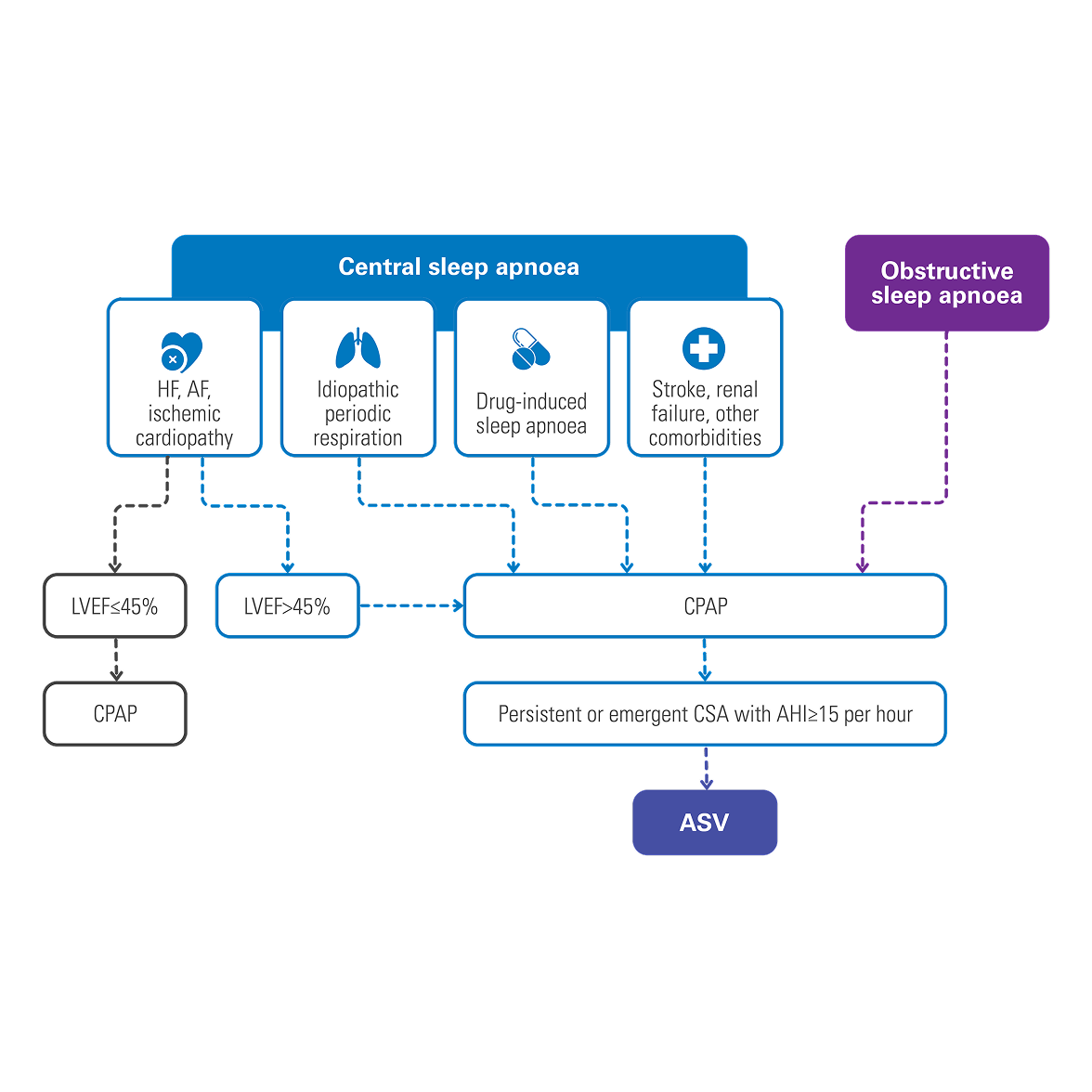
When can ASV therapy be prescribed?
The ERS statement about the treatment of central breathing disturbances during sleep.4
Understand how our ASV algorithm works

Central sleep apnea

Periodic breathing
ASV better than CPAP at controlling respiratory events in patients with CompSA
In an intention-to-treat analysis, success (apnoea hypopnoea index [AHI] < 10) at 90 days of therapy was achieved in 89.7% of patients treated with ASV versus 64.5% of participants treated with CPAP.6
[N = 66, prospective randomised trial]

ASV decreases residual sleepiness after APAP therapy in patients with mixed sleep apnoea
After 30 days of APAP treatment, ASV provided a further reduction (compared to baseline) of 12.9% in AHI, 48.5% in central sleep apnoea index (CSAI), 26.1% in micro-arousal index (MAI), and 37.9% in Epworth Sleepiness Scale (ESS) score at similar mean pressure.7
[N = 42, sequential study]
ASV better than bi-level ST at reducing respiratory events in opioid-induced CSA
In opioid-induced CSA, ASV therapy reduced AHI by 84.7%, central apnoea index (CAI) by 95.7%, Apnoea Index (AI) by 96.4%, and respiratory arousal index (RAI) by 77.1% when compared to bi-level ST. Respiratory parameters were normalised in 83.3% of patients on ASVAuto but only 33.3% of patients on bi-level ST.8
[N = 18, prospective, randomised crossover polysomnography study]
ASV improves AHI and ESS in post-acute ischemic stroke patients
ASV therapy improved outcomes for post-acute ischemic stroke patients with CSA, reducing AHI by 81.8% and ESS by 35.6%.9
[N = 15, single centre retrospective analysis]
CPAP, APAP and bilevel therapy
Positive airway pressure therapy can be delivered in a number of modes:
- Continuous positive airway pressure (CPAP), which delivers air at a fixed pressure.
- Automatic positive airway pressure (APAP), which automatically adjusts pressure levels based on a patient's breathing. APAP may be suitable for patients with REM-related sleep apnea, positional apnea or who experience non-compliance with standard CPAP therapy.
- Bilevel therapy, which provides higher inspiratory pressure (IPAP) and lower expiratory pressure (EPAP) - can also be effective for certain OSA patients who are non-compliant, and used to treat a wide-range of sleep and respiratory disordered breathing other than OSA such as include CSA, overlap syndrome, COPD, and more.
Patient outcomes and comorbidities
Helping your patients start and continue with the most effective sleep apnea treatment can help them regain control of their lives. Effective treatment has been shown to reverse the effects of daytime sleepiness, fatigue, moodiness and depression. And studies have shown that when patients are successful with their therapy, their long-term health care costs are at least 50% lower overall.1
There are also a variety of serious comorbidities such as cardiovascular disease, diabetes and stroke that have a strong connection to sleep apnea.
ASV therapy from a patient and physician perspective

Resmed ASV patient Fred Schouwenaars
Discover Fred Schouwenaars’s story, a patient with central sleep apnoea. He’s joined by his Sleep Physician, Prof. Venekamp, Pulmonologist and Sleep Physician at the Institute Kempenhaeghe in the Netherlands.

Resmed ASV physician
Watch Professor Venekamp, Pulmonologist and Sleep Physician at the Institute Kempenhaeghe in the Netherlands, talk about her experience with adaptive-servo ventilation therapy and her patient Fred Schouwenaars.

Resmed ASV Professor Pépin
Watch Professor Pépin, Head of Sleep Laboratory in Grenoble, France, share clinical updates about adaptive-servo ventilation therapy.
Looking for more information about CSA and ASV?

AirCurve 11 ASV
