


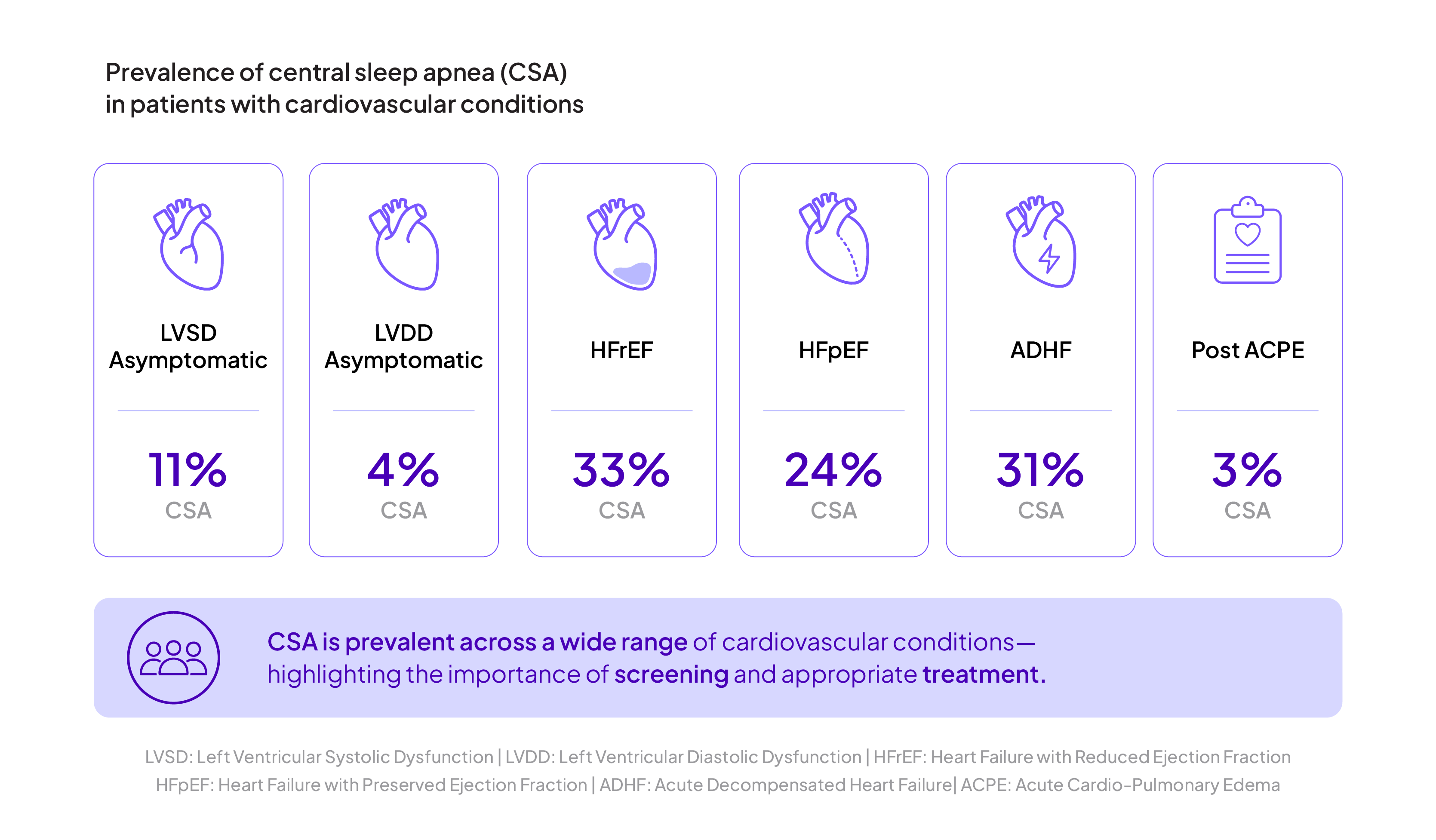
CSA prevalence in cardiovascular disease (CVD) patients:5
ASV improves outcomes
Recent research, including registries and large cohort studies, has shown the positive effects of ASV therapy on the CSA patient population.6,7

Sleep improvement (PSQI, FOSQ)

Disease-specific QoL improvement (SF - 36, Pichot Fatigue Scale)

Reduced sleepiness


How to treat patients with central sleep apnea
Discover how Resmed's adaptive Servo-Ventilation (ASV) solution promotes harmony, safety and comfort.

CPAP, APAP and bilevel therapy
Positive airway pressure therapy can be delivered in a number of modes:
- Continuous positive airway pressure (CPAP), which delivers air at a fixed pressure.
- Automatic positive airway pressure (APAP), which automatically adjusts pressure levels based on a patient's breathing. APAP may be suitable for patients with REM-related sleep apnea, positional apnea or who experience non-compliance with standard CPAP therapy.
- Bilevel therapy, which provides higher inspiratory pressure (IPAP) and lower expiratory pressure (EPAP) - can also be effective for certain OSA patients who are non-compliant, and used to treat a wide-range of sleep and respiratory disordered breathing other than OSA such as include CSA, overlap syndrome, COPD, and more.

Patient outcomes and comorbidities
Helping your patients start and continue with the most effective sleep apnea treatment can help them regain control of their lives. Effective treatment has been shown to reverse the effects of daytime sleepiness, fatigue, moodiness and depression. And studies have shown that when patients are successful with their therapy, their long-term health care costs are at least 50% lower overall.1
There are also a variety of serious comorbidities such as cardiovascular disease, diabetes and stroke that have a strong connection to sleep apnea.